Lump on Neck or Back of Neck: Information to Know
Radiation therapy to the neck may change the way the thyroid gland works. Blood tests may be done to check the thyroid hormone level in the body before treatment and at regular checkups after treatment.
Metastatic Squamous Neck Cancer with Occult Primary Treatment (Adult) (PDQ®)–Patient Version
General Information About Metastatic Squamous Neck Cancer with Occult Primary
Key Points
- Metastatic squamous neck cancer with occult primary is a disease in which squamous cell cancer spreads to lymph nodes in the neck and it is not known where the cancer first formed in the body.
- Signs and symptoms of metastatic squamous neck cancer with occult primary include a lump or pain in the neck or throat.
- Tests that examine the tissues of the neck, respiratory tract, and upper part of the digestive tract are used to detect (find) and diagnose metastatic squamous neck cancer and the primary tumor.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Metastatic squamous neck cancer with occult primary is a disease in which squamous cell cancer spreads to lymph nodes in the neck and it is not known where the cancer first formed in the body.
Squamous cells are thin, flat cells found in tissues that form the surface of the skin and the lining of body cavities such as the mouth, hollow organs such as the uterus and blood vessels, and the lining of the respiratory (breathing) and digestive tracts. Some organs with squamous cells are the esophagus, lungs, kidneys, and uterus. Cancer can begin in squamous cells anywhere in the body and metastasize (spread) through the blood or lymph system to other parts of the body.
When squamous cell cancer spreads to lymph nodes in the neck or around the collarbone, it is called metastatic squamous neck cancer. The doctor will try to find the primary tumor (the cancer that first formed in the body), because treatment for metastatic cancer is the same as treatment for the primary tumor. For example, when lung cancer spreads to the neck, the cancer cells in the neck are lung cancer cells and they are treated the same as the cancer in the lung. Sometimes doctors cannot find where in the body the cancer first began to grow. When tests cannot find a primary tumor, it is called an occult (hidden) primary tumor. In many cases, the primary tumor is never found.
Signs and symptoms of metastatic squamous neck cancer with occult primary include a lump or pain in the neck or throat.
Check with your doctor if you have a lump or pain in your neck or throat that doesn’t go away. These and other signs and symptoms may be caused by metastatic squamous neck cancer with occult primary. Other conditions may cause the same signs and symptoms.
Tests that examine the tissues of the neck, respiratory tract, and upper part of the digestive tract are used to detect (find) and diagnose metastatic squamous neck cancer and the primary tumor.
Tests will include checking for a primary tumor in the organs and tissues of the respiratory tract (part of the trachea), the upper part of the digestive tract (including the lips, mouth, tongue, nose, throat, vocal cords, and part of the esophagus), and the genitourinary system.
The following procedures may be used:
The per capita price of healthcare per year is higher in the United States than in any other nation in the world, according to National Public Radio (NPR). America spends nearly 2.5 times as much per person as the United Kingdom does, despite having comparable wealth and a lower life expectancy.
- Physical exam and health history: An exam of the body, especially the head and neck, to check general signs of health. This includes checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist or tested in the laboratory to check for signs of cancer. Three types of biopsy may be done:
- Fine-needle aspiration (FNA) biopsy: The removal of tissue or fluid using a thin needle.
- Core needle biopsy: The removal of tissue using a wide needle.
- Excisional biopsy: The removal of an entire lump of tissue.
The following procedures are used to remove samples of cells or tissue:
- Tonsillectomy: Surgery to remove both tonsils.
- Endoscopy: A procedure to look at organs and tissues inside the body to check for abnormal areas. An endoscope is inserted through an incision (cut) in the skin or opening in the body, such as the mouth or nose. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove abnormal tissue or lymph node samples, which are checked under a microscope for signs of disease. The nose, throat, back of the tongue, esophagus, stomach, voice box, windpipe, and large airways will be checked.
One or more of the following laboratory tests may be done to study the tissue samples:
- Immunohistochemistry: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient’s blood or bone marrow. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the blood or bone marrow, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
- Light and electron microscopy: A test in which cells in a sample of tissue are viewed under regular and high-powered microscopes to look for certain changes in the cells.
- Epstein-Barr virus (EBV) and human papillomavirus (HPV) test: A test that checks the cells in a sample of tissue for EBV and HPV DNA.
A diagnosis of occult primary tumor is made if the primary tumor is not found during testing or treatment.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on the following:
- The number and size of lymph nodes that have cancer in them.
- Whether the cancer has responded to treatment or has recurred (come back).
- How different from normal the cancer cells look under a microscope.
- The patient’s age and general health.
Treatment options also depend on the following:
- Which part of the neck the cancer is in.
- Whether certain tumor markers are found.
Stages of Metastatic Squamous Neck Cancer with Occult
Primary
Key Points
- After metastatic squamous neck cancer with occult primary has been diagnosed, tests are done to find out if cancer cells have spread to other parts of the body.
- There are three ways that cancer spreads in the body.
- Metastatic squamous neck cancer with occult primary can recur (come back) after it has been treated.
After metastatic squamous neck cancer with occult primary has been diagnosed, tests are done to find out if cancer cells have spread to other parts of the body.
The process used to find out if cancer has spread to other parts of the body is called staging. There is no standard staging system for metastatic squamous neck cancer with occult primary.
The results from tests and procedures used to detect and diagnose the primary tumor are also used to find out if cancer has spread to other parts of the body.
The tumors are described as untreated or recurrent. Untreated metastatic squamous neck cancer with occult primary is cancer that is newly diagnosed and has not been treated, except to relieve signs and symptoms caused by the cancer.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Metastatic squamous neck cancer with occult primary can recur (come back) after it has been treated.
The cancer may come back in the neck or in other parts of the body.
Treatment Option Overview
Key Points
- There are different types of treatment for patients with metastatic squamous neck cancer with occult primary.
- Two types of standard treatment are used:
- Surgery
- Radiation therapy
- Chemotherapy
- Hyperfractionated radiation therapy
There are different types of treatment for patients with metastatic squamous neck cancer with occult primary.
Different types of treatment are available for patients with metastatic squamous neck cancer with occult primary. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Two types of standard treatment are used:
Surgery
Surgery may include neck dissection. There are different types of neck dissection, based on the amount of tissue that is removed.
- Radical neck dissection: Surgery to remove tissues in one or both sides of the neck between the jawbone and the collarbone, including the following:
- All lymph nodes.
- The jugular vein.
- Muscles and nerves that are used for face, neck, and shoulder movement, speech, and swallowing.
After the doctor removes all the cancer that can be seen at the time of surgery, some patients may be given radiation therapy after surgery to kill any cancer cells that are left. Treatment given after surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
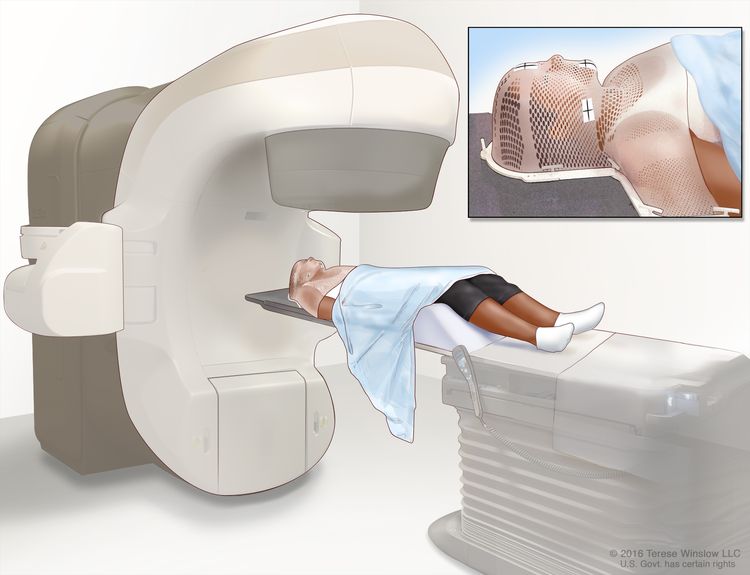
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. Intensity-modulated radiation therapy (IMRT) is a type of 3-dimensional (3-D) external radiation therapy that uses a computer to make pictures of the size and shape of the tumor. Thin beams of radiation of different intensities (strengths) are aimed at the tumor from many angles. This type of radiation therapy is less likely to cause dry mouth, trouble swallowing, and damage to the skin.
Radiation therapy to the neck may change the way the thyroid gland works. Blood tests may be done to check the thyroid hormone level in the body before treatment and at regular checkups after treatment.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy).
Hyperfractionated radiation therapy
Hyperfractionated radiation therapy is a type of external radiation treatment in which a smaller than usual total daily dose of radiation is divided into two doses and the treatments are given twice a day. Hyperfractionated radiation therapy is given over the same period of time (days or weeks) as standard radiation therapy.
Treatment for metastatic squamous neck cancer with occult primary may cause side effects.
For information about side effects caused by treatment for cancer, see our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Treatment of Untreated Metastatic Squamous Neck Cancer with Occult Primary
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of untreated metastatic squamous neck cancer with occult primary may include the following:
- Radiation therapy.
- Surgery.
- Radiation therapy followed by surgery.
- A clinical trial of chemotherapy followed by radiation therapy.
- A clinical trial of chemotherapy given at the same time as hyperfractionated radiation therapy.
- Clinical trials of new treatments.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Recurrent Metastatic Squamous Neck Cancer with Occult Primary
For information about the treatments listed below, see the Treatment Option Overview section.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
To Learn More About Metastatic Squamous Neck Cancer with Occult Primary
For more information from the National Cancer Institute about metastatic squamous neck cancer with occult primary, see the following:
- Carcinoma of Unknown Primary Home Page
- Head and Neck Cancer Home Page
- Oral Complications of Chemotherapy and Head/Neck Radiation
- Metastatic Cancer
For general cancer information and other resources from the National Cancer Institute, see the following:
- About Cancer
- Staging
- Chemotherapy and You: Support for People With Cancer
- Radiation Therapy and You: Support for People With Cancer
- Coping with Cancer
- Questions to Ask Your Doctor about Cancer
- For Survivors and Caregivers
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute’s (NCI’s) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of adult metastatic squamous neck cancer with occult primary. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary (“Updated”) is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become “standard.” Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI’s website. For more information, call the Cancer Information Service (CIS), NCI’s contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Metastatic Squamous Neck Cancer with Occult Primary Treatment (Adult). Bethesda, MD: National Cancer Institute. Updated . Available at: https://www.cancer.gov/types/head-and-neck/patient/adult/metastatic-squamous-neck-treatment-pdq. Accessed . [PMID: 26389176]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
If you would like to reproduce some or all of this content, see Reuse of NCI Information for guidance about copyright and permissions. In the case of permitted digital reproduction, please credit the National Cancer Institute as the source and link to the original NCI product using the original product’s title; e.g., “Metastatic Squamous Neck Cancer with Occult Primary Treatment (Adult) (PDQ®)–Patient Version was originally published by the National Cancer Institute.”
Want to use this content on your website or other digital platform? Our syndication services page shows you how.
Lump on Neck or Back of Neck: Information to Know
The first thing you should know is that most neck lumps are not a sign of cancer. There are a host of more common causes of neck lumps, including infections, cysts, boils, and other common skin irritations.
However, a neck lump can also be an early sign of several types of cancer, so if your lump does not go away in a week or two, you should consult with your doctor. If your neck lump is caused by a swollen lymph node, it could be cancerous — but again, this is far from the most likely explanation.
What are the lymph nodes and how are they related to neck lumps?
Lymph nodes are key components of the body’s immune system. These small, bean-shaped capsules are located throughout the body and are responsible for filtering and removing harmful substances from your body. Hundreds of lymph nodes are connected by a vascular system that transports white blood cells, which help fight infections by attacking germs, bacteria, and diseases. This is similar to the system that transports blood.
The most common cause of swollen lymph nodes is that they are fighting an infection, which indicates that they are operating effectively as part of your immune system. If this is the cause, the swelling will disappear as soon as the infection is defeated.
Can a neck lump or swollen lymph nodes be a sign of cancer?
In rare cases, swollen lymph nodes can be the first sign of cancer. Unlike a lump caused by infection, a cancerous lump will rarely disappear. Therefore, if the lump persists for more than a week or so, you should consult your doctor. (Other significant ailments can cause the lymph nodes to swell, including strep throat, mononucleosis, tonsilitis, and HIV.)
“Feeling a lump in your neck is not a reason to panic,” says Kartik Sehgal, MD, a head and neck medical oncologist and director of the Thyroid Cancer Center at Dana-Farber Brigham Cancer Center. “While the majority of lumps are benign, it’s important to report persistent lumps and associated symptoms to your doctor.”
What does a cancerous neck lump feel like?
Cancerous lymph nodes can occur anywhere on the neck and are typically described as hard rather than squishy like the swollen nodes caused by infection. The lumps can range in size from a half-inch to several inches in diameter.
While you may only notice a single lump, it is not uncommon to find them clumped together, spread out along one side of the neck, or even along both sides of the neck depending on the location of a possible tumor. Although they are usually painless, some cancerous lymph nodes can become painful after drinking alcohol.
In the case of cancer, the lump occurs when cancer cells infiltrate the lymph capsule and multiply rapidly. If left untreated, cancer can break out of the lymph node and spread to other parts of the body.
What types of cancer might a neck lump indicate?
A neck lump is often the only symptom of head and neck cancer, which is why it’s important to monitor lumps and consult your doctor if they don’t go away. The types of cancer that are most frequently associated with neck lumps are:
- Lymphoma, which falls into two broad categories, Hodgkin lymphoma and non-Hodgkin lymphoma. Both are cancers of the lymphatic system which fight infection and disease. A swollen lymph node is the most common, and often the earliest, symptom of lymphoma.
- Leukemia is a general term for blood cancer. Leukemia generally begins in the bone marrow and can often result in swollen lymph nodes.
- Thyroid cancer occurs in the butterfly-shaped gland at the front base of your neck. This gland produces hormones to regulate heart rate, blood pressure, and weight. A lump caused by thyroid cancer will most likely be located at the front of your neck below the voice box. While 80 to 90 percent of reported thyroid lumps are not cancerous, it’s important to inform your healthcare provider if you notice any changes.
- Any metastasized cancer that has spread beyond its place of origin and entered the lymphatic system.
How is a cancerous lymph node diagnosed?
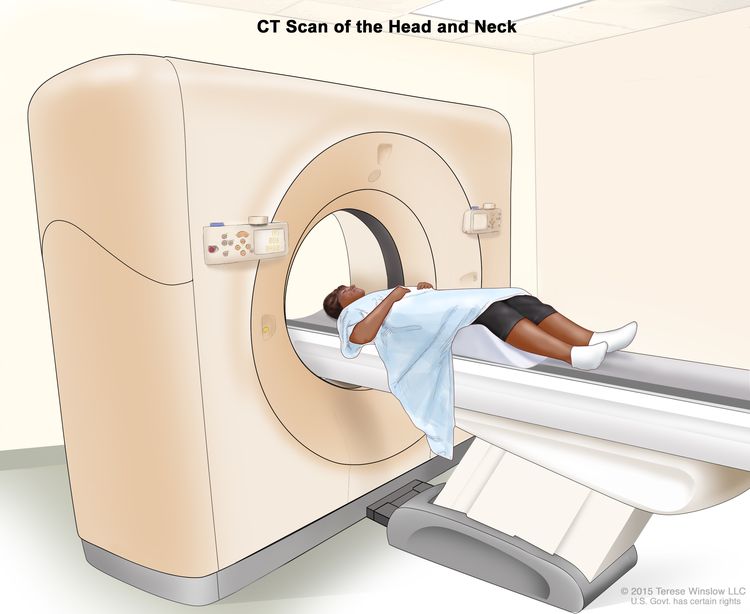
If your lymph node has been swollen for several weeks, a biopsy may be required to determine if it is cancerous. The biopsy may be done by surgically removing the node, or by inserting a needle to take a smaller sample. If cancer is found, doctors may use various imaging technologies (X-ray, CT scan, PET scan, or MRI) to determine if the cancer originated in the lymph node or metastasized from another part of your body.
Other than cancer, what can cause a neck lump?
In addition to swollen lymph nodes, there are a variety of ailments that can cause lumps beneath the skin of the neck and aren’t usually related to cancer, including:
- Thyroid nodules are lumps that live under the skin in the front of the neck. They can either be fluid-filled or solid and are usually harmless. In rare cases, thyroid lumps can prove to be cancerous.
- An infection below the surface of the skin.
- A cyst, which is a slow-growing bump under the skin, has a smooth surface and is usually painless. Cysts are usually not cause for concern unless they become infected or grow very large. Sometimes cysts can emit a thick, yellow, smelly fluid.
- Boils are typically caused by a bacterial or fungal infection due to a blocked hair follicle or oil gland. Although they can appear anywhere, they are often found on the neck. Boils are red and painful lumps with a yellow or white center. They are caused by a localized infection that rarely spreads beyond the boil itself. They may rupture and weep fluid. You should not squeeze or prick a boil since this can cause the infection to become worse or spread. Instead, apply warm compresses and keep the area clean.
- An allergic reaction to many substances can irritate the neck, including detergent residue, shampoo, and sunscreen. Lumps caused by an allergic reaction are often itchy or painful.
- Muscle knots, including on the back of the neck, from injury, overuse, or tension. These knots can be as small as a pea or as large as a baseball. They are typically invisible since they remain beneath the skin and don’t cause lumps. It will often be painful to push on a muscle knot, whereas a cancerous lymph node is rarely painful.
- Lipoma is a fatty tissue deposit that is not painful and is unlikely to cause other problems.
- Mononucleosis is caused by infection with a contagious virus that can last months. It can cause swollen lymph nodes in addition to the more widely known symptoms such as extreme fatigue, fever, sore throat, and headaches.
About the Medical Reviewer
Dr. Sehgal completed his fellowship training in hematology and medical oncology at Beth Israel Deaconess Medical Center, a Harvard Medical School teaching hospital, in 2020. Prior to this, he earned his medical degree from the All India Institute of Medical Sciences, New Delhi, and finished residency training in internal medicine at Yale-New Haven Hospital, CT. Dr. Sehgal’s research interests are in the fields of translational immuno-oncology and experimental therapeutics. He has previously trained in the Dhodapkar Laboratory at Yale University and Barbie Laboratory at Dana-Farber Cancer Institute. His research has led to publications in scientific journals such as Science Translational Medicine, Nature Medicine, Blood and Journal of Immunology. He is currently engaged in clinical and translational research directed towards delineating mechanisms of therapeutic resistance to immune checkpoint inhibitors and developing more effective combinations with molecularly targeted therapies.
Make an Appointment or Get a Second Opinion
Boston (Main Campus)
Adults: 877-442-3324
Pediatric: 888-733-4662Our Online Second Opinion program lets adult patients from all over the world receive expert second opinions from Dana-Farber oncologists without leaving home.
Get A Weekly Insight Email
About Our Patient Stories
Dana-Farber shares patient stories which may include descriptions of actual medical results. Dana-Farber provides personalized care for each patient based on their unique needs; their experiences and results will vary.
Why You Can Trust Insight
Insight is committed to bringing you information about cancer that you can trust and that meets the highest editorial and scientific standards. We employ a strict editorial process to ensure that what you read is factually correct. Learn more about our process here.